

Health
Monkeypox Q&A: how do you catch it and what are the risks? An expert explains
THE LATEST outbreak of monkeypox has, at the time of writing, reached 17 countries with 110 confirmed cases and a further 205 suspected cases. It’s a fast-moving story, so if you need to catch up on the latest, here are answers to some of the most pressing questions.
How is monkeypox spreading?
The first patient in the current outbreak had returned to the UK from travels to Nigeria where monkeypox is endemic. However, cases are now spreading among people who have not travelled to west or central Africa, suggesting local transmission is occurring.
Monkeypox usually spreads by close contact and respiratory droplets. However, sexual transmission (via semen and/or vaginal fluid) has been posited as an additional possible route. The World Health Organization (WHO) says: “Studies are needed to better understand this risk.”
Most cases in the current outbreak have been in youngish men, but the virus can spread to anyone.
There are no confirmed cases in Pembrokeshire at the present time.
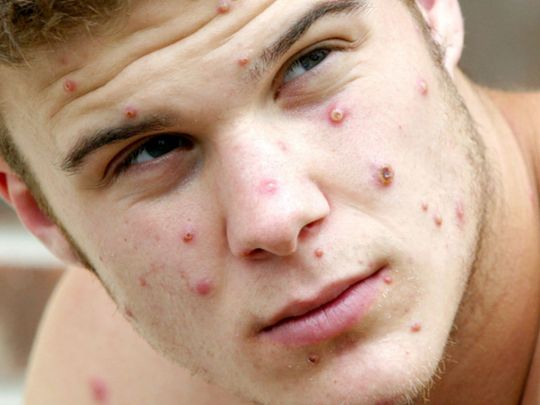
What are the symptoms?
Early symptoms are flu-like, such as a fever, headaches, aching muscles and swollen lymph nodes.
Once the fever breaks, a rash can develop, often beginning on the face and then spreading to other parts of the body – most commonly the palms of the hands and soles of the feet.
How deadly is monkeypox?
Monkeypox is mostly a mild, self-limiting disease lasting two-to-three weeks. However, in some cases, it can cause death. According to the WHO, the fatality rate “in recent times” has been around 3% to 6%. The west African monkeypox virus is considered to be milder than the central African one.
Monkeypox tends to cause more serious disease in people who are immunocompromised – such as those undergoing chemotherapy – and children. There have been no deaths from monkeypox in the current worldwide outbreak, but, according to the Daily Telegraph, one child in the UK is in intensive care with the disease.

Why is it called monkeypox?
Monkeypox was first identified in laboratory monkeys (macaques) in Denmark in 1958, hence the name. However, monkeys don’t seem to be the natural hosts of the virus. It is more commonly found in rats, mice and squirrels. The first case in humans was seen in the 1970s in the Democratic Republic of the Congo.
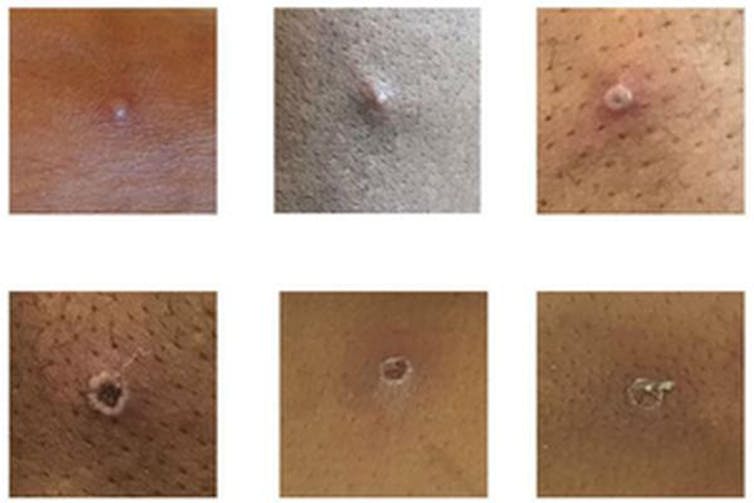
Is monkeypox related to smallpox and chickenpox?
Monkeypox is related to smallpox – they are both orthopoxviruses – but it is not related to chickenpox. Despite the name, chickenpox is a herpes virus, not a poxvirus. (How “chicken” got in the name is not entirely clear. In his dictionary of 1755, Samuel Johnson surmised that it is so named because it is “of no very great danger”.) Nevertheless, the vesicles (little pus-filled blisters) caused by monkeypox are similar in appearance to those of chickenpox.
Are cases likely to continue rising?
Cases are likely to continue to rise significantly over the next two-to-three weeks, but this is not another pandemic in the making. Monkeypox doesn’t spread anywhere near as easily as the airborne virus SARS-CoV-2 that causes COVID-19.
Has monkeypox evolved to be more virulent?
RNA viruses, such as SARS-CoV-2, don’t have the ability to check their genetic code for mistakes each time they replicate, so they tend to evolve faster. Monkeypox is a DNA virus, which does have the ability to check itself for genetic mistakes each time it replicates, so it tends to mutate a lot slower.
The first genome sequence of the current outbreak (from a patient in Portugal) suggests that the virus is very similar to the monkeypox strain that was circulating in 2018 and 2019 in the UK, Singapore and Israel. So it is unlikely that the current outbreak is the result of a mutated virus that is better at spreading.
How is monkeypox diagnosed?
In the UK, swab samples taken from the patient are sent to a specialist laboratory that handles rare pathogens, where a PCR test is run to confirm monkeypox. The UK Health Security Agency has only one rare and imported pathogens laboratory.
Is there a vaccine for it?
Vaccines for smallpox, which contain the lab-made vaccinia virus, can protect against monkeypox. However, the vaccine that was used to eradicate smallpox can have severe side-effects, killing around one in a million people vaccinated.
The only vaccine specifically approved for monkeypox, Imvanex, is made by a company called Bavarian Nordic. It uses a nonreplicating form of vaccinia, which causes fewer side-effects. It was approved by the US Food and Drug Administration and the European Medicines Agency in 2019 – but only for use in people 18 years of age or older.
UK health secretary Sajid Javid said that the UK government will be stocking up on vaccines that are effective against monkeypox. The UK currently has about 5,000 doses of smallpox vaccine, which has an efficacy of around 85% against monkeypox.
Are there drugs to treat it?
There are no specific drugs to treat monkeypox. However, antivirals such as cidofovir and brincidofovir have been proven to be effective against poxviruses in animals and may also be effective against monkeypox infections in humans.
By Ed Feil, Professor of Microbial Evolution at The Milner Centre for Evolution, University of Bath
This article is republished from The Conversation under a Creative Commons license. Read the original article.

PATIENTS are facing some of the worst medicine shortages ever seen in the UK, with pharmacists warning the situation now poses a serious risk to safety.
The National Pharmacy Association said shortages affecting commonly used medicines are becoming more frequent, lasting longer, and causing increasing disruption for patients, GP surgeries and pharmacies.
The warning comes as Serious Shortage Protocols for Creon, used by people with pancreatic cancer and cystic fibrosis to help digest food, have been in place since May 2024 and have now been extended until July 10, 2026.
HRT treatment Estradot has also been under a Serious Shortage Protocol since December 2024, with the current extension also running until July 10.
Patients travelling between pharmacies
A survey by the National Pharmacy Association found that 98 per cent of pharmacies had encountered patients who had visited several pharmacies in one day to find a prescription.
It also found that 96 per cent of pharmacies believed the current situation posed a serious risk to patient safety, while 89 per cent said they had been unable to dispense a medicine at least once a day because of supply problems.
Some pharmacy teams have also faced anger and abuse from patients unable to obtain medication.
Olivier Picard, Chair of the National Pharmacy Association, said: “Medicine shortages are becoming more frequent, lasting longer and causing increasing disruption for patients.
“These shortages are some of most severe the UK has experienced.
“It is deeply distressing to find patients who have travelled from pharmacy to pharmacy to find the medicines they need without success.”
Calls for urgent taskforce
The NPA is calling on the government to convene an emergency taskforce involving manufacturers, wholesalers, clinicians and pharmacists.
It also wants changes to rules which currently stop pharmacists from making simple substitutions, such as changing a tablet to a capsule or a cream to an ointment, even where a safe alternative is available.

Professor Victoria Tzortziou Brown, President of the Royal College of GPs, said medicine shortages were frustrating for patients, GPs and pharmacists, and added pressure to already stretched services.
She said the College supported pharmacists being able to make limited changes to prescriptions where a medicine is unavailable and a safe alternative exists.
She added: “The most important thing is that patients are able to access the medication they need safely and without delay.”
The Cystic Fibrosis Trust and Pancreatic Cancer UK have also raised concerns about the impact of shortages of pancreatic enzyme replacement therapy, including Creon, on people who rely on the medication to digest food, maintain weight and stay well enough for treatment.

A CARMARTHEN woman has been jailed after admitting a lengthy catalogue of offences including assaults on police officers, harassment, breaching a Community Protection Notice, shop theft, possession of an XL Bully dog and assaulting a paramedic.
Tilly Rees, 25, of Llys Caermedi, Carmarthen, appeared before Llanelli Magistrates’ Court on Wednesday (Jun 18).
The court heard that Rees admitted multiple breaches of a Community Protection Notice issued in 2025, including incidents in which she shouted abuse in public, caused distress to residents and repeatedly targeted individuals named in court proceedings.
Harassment campaign
Among the offences was a harassment charge relating to a course of conduct against a Carmarthen man between March and May this year.
Prosecutors said Rees approached him on multiple occasions, shouted abuse, called him a paedophile and video-recorded him and his home.
She also admitted a series of Community Protection Notice breaches linked to the same behaviour.
Police assaults
The court heard that Rees assaulted a number of police officers during incidents in Llanelli on May 1 and May 5.
Several assault charges against serving police constables were taken into account by the court when sentence was passed.
A further charge of assaulting a paramedic at Dafen Police Station on June 12 was also admitted.
Shop theft and XL Bully
Rees also admitted stealing items including sanitary products, deodorant, skincare products and reading glasses from a Carmarthen pharmacy.
In a separate matter, she admitted possessing an XL Bully dog contrary to the Dangerous Dogs Act. The court ordered the dog to be forfeited and destroyed after Rees relinquished her rights to it.
Restraining orders imposed
District Judge M Layton imposed a number of restraining orders preventing Rees from contacting named individuals or referring to them online.
The orders prohibit direct or indirect contact and restrict social media activity relating to those protected by the orders.
Jailed for 26 weeks
Magistrates concluded that only an immediate custodial sentence could be justified.
Rees was sentenced to a total of 26 weeks’ imprisonment.
The court heard that some of the offences were committed while she was already subject to a suspended sentence, while others involved assaults on emergency workers carrying additional aggravating factors.

COMMENTS made by a Reform MS led to a walkout in the Senedd during a debate on the Welsh Government’s international spending.
A Reform motion, calling for an end to all Welsh Government international spending, was rejected by Senedd Members on Wednesday June 17.
Wednesday’s plenary opened with Llywydd Huw Irranca-Davies reminding members to mind their language and tone when contributing, following clashes between Reform UK’s Joe Martin and the First Minister in Tuesday’s proceedings.
Mr Irranca-Davies said: “Robust disagreement is part of democratic debate, but it must always be grounded in respect and we must avoid using language that has the potential to inflame debate or to increase tensions.”
The debate was opened by Reform’s shadow minister for finance and government efficiency, Cai Parry-Jones, but it was the contribution made by Caerdydd Penarth MS Joe Martin which sparked the most controversy.

Announcing to his colleagues that he had “good news”, Mr Martin began his statement by sharing that he had “found the £9 million” needed for Plaid’s “childcare idea”.
However, Mr Martin then added that the “bad news” was to get the money the government would have to stop funding “some of the most pointless schemes known to man”.
One example Mr Martin gave of these so-called “pointless schemes” was a beekeeping scheme in Uganda designed to advance gender equality.
The scheme, run by Bees for Development and their partner organisation, The Uganda National Apiculture Development Organisation, aimed to enhance women’s economic empowerment through beekeeping.
It challenged gender norms in the industry, increasing the visibility of women in technical and policy leaderships roles.
Mr Martin then suggested Wales had won the “Who can find the stupidest use of taxpayer money?” competition because of a scheme supporting tree planting in Uganda.
He said: “We actually asked some Ugandan people what they thought about Wales’s scheme to send them money for trees and they said, ‘Why are you sending us money for trees?’

“We then asked the same question to some Welsh students who had been through our underfunded education system, but we didn’t get a reply because we had e-mailed them and they couldn’t read.”
Mr Martin went on to criticise the money spent on mini embassies abroad.
He said: “In India, one of the functions of those mini embassies is to recruit nurses to come and work in our NHS, which is great because it means that the Welsh people who would have otherwise become nurses can instead go on universal credit.”
The Reform MS then added: “I have enquired as to why we can’t just have an enormous pit where we burn all the money, but apparently that’s not compliant with net zero.”
At this point in Mr Martin’s statement Plaid Cymru’s Zaynub Akbar, of Caerdydd Ffynnon Taf, announced she was going to leave the Siambr.
She said: “I don’t accept any of this and I don’t want to be a part of it, so I’ll be leaving the chamber.”

She was followed by numerous other Senedd Members, including Trefnydd and chief whip Heledd Fychan.
Mr Martin was then reminded by the Llywydd of Senedd rules, which mandate respect in the chamber, before he could continue his contribution.
He concluded his speech to the Senedd by saying: “In Westminster, the Tory party doubled foreign aid whilst imposing austerity. There are now only seven of them in this chamber. The same fate awaits any party that insults taxpayers by frittering money overseas on feel-good vanity projects.
“So, I want to encourage the Party of Wales to be nationalist, to put Wales first. Spend your constituents’ money on your constituents. That way, when someone is lying in a hospital corridor and they ask you, ‘are you really the Party of Wales?’, you’ll be able to say ‘yes’.”
At the end of the debate, the Llywydd directly addressed Mr Martin calling for him to “reflect” on his remarks and contributions, noting that it was “not in line with [his] expectations”.
Mr Irranca-Davies described it as “particularly disappointing” given the comments he made at the beginning of plenary.
He said: “Going forward, I think we all need to reflect on this and make sure that we comply with our conduct within this chamber and the way we comport ourselves in light of my remarks.”
Welsh Conservative leader Darren Millar expressed his support for the Reform-backed motion, saying it is a debate about where responsibilities lie.
He said: “It’s very clear that foreign relations, international development are matters for the UK Government, not the Welsh Government, and as a result of that, I believe that we respect devolution and can expect respect for devolution back when we respect the boundaries of our legislative competence and the competence of the Welsh Government’s position as well.”

Mr Millar highlighted that his party has continuously argued against the development of “mini embassies” and “overseas offices”.
The Conservative leader did clarify however that he is not “anti-international aid”, and noted the “generous” nature of the people of Wales.
But he added: “I do not believe that when people are dying waiting for ambulances, when we’re at the bottom of the educational tree as far as the league table of the United Kingdom is concerned, and when our road infrastructure isn’t working, our transport infrastructure is creaking, that it’s right to spend those millions of pounds on those things, when the Welsh Government should be focused on the things for which it is responsible.”
Taking an intervention from Labour’s Huw Thomas, Mr Millar was questioned on whether he recognises that the majority of international spending is on economic development for Wales.

Mr Millar once again referred to the role of the UK Government, noting that it is their responsibility to bring inward investment to the UK as a whole.
He said: “We will always want to be an internationalist country, looking out and seeking to influence the world, but we do that as part of the United Kingdom, an integral part of the United Kingdom.
“And I’m proud to be a member not only of the Welsh Conservative Party, but of the Conservative and Unionist Party, and I believe in the union of the United Kingdom, and that these foreign relationships and international development are done better as a United Kingdom as a whole.”
Plaid Cymru’s Gwyn Williams shared a notably different perspective to that of his Conservative and Reform colleagues.
Prior to being elected to the Senedd, Dr Williams was a consultant ophthalmologist specialising in retina care at Swansea Bay University Health Board.

Speaking as someone who has worked within the Welsh NHS Dr Williams said: “Wales has long been a country that looks beyond our own horizons, looking to make a difference in the world and help where we can, but also we rely on help coming in to us as well.
“Many, many healthcare workers, of course, come from abroad, especially here in Wales, and every hospital in the country would crumble if all the international workers went home.”
He continued: “In Singleton Hospital in Swansea, in the eye department, I am the only Welsh-speaking, Welsh-origin consultant there, and much as I like to convince myself that I can do the work of ten people, I cannot, especially now because I am here.
“Chronic shortages in these sectors increase hospital discharge delays, reduce bed availability and create bottlenecks across the healthcare system.
“At a time when the NHS is struggling, we need the support from abroad as well, though we also, of course, need to grow our own ability.”
Concluding his statement Dr Williams said: “This whole debate tries to position international investment and domestic investment as a zero-sum game. It isn’t.
“Looking outwards does not come at the expense of looking inwards. I suggest that such a simplistic outlook condescends to the people of Wales and stymies science.”

The cabinet minister for government effectiveness, Dafydd Trystan Davies, called for reflection on the tone of the debate, suggesting that the “standard of this debate [had] descended to the level of a public house, not of a national Senedd”.
He said: “My friend the leader of the Welsh Conservatives made a speech, and I disagree with more or less all of it, and yet it was conducted properly and in line with the standing orders and the procedures of this Senedd.
“I think we should all take our duties properly as parliamentarians, whatever views we agree or disagree on.”
Dr Trystan Davies highlighted that international spending makes up just 0.03% of the Welsh Government’s overall budget, which he described as a “small contribution” to “building our prosperity, protecting our public services, strengthening our culture, and promoting our values”.
He said: “Our international work turns that belief into action, creating jobs and investment, exports and partnerships, life-changing experiences for students, new colleagues for our NHS and enabling communities in Wales and beyond to learn from one another.
“When Wales works internationally, Welsh people benefit. Our businesses reach new markets, universities build global partnerships, young people return home with skills and confidence, and Wales’s reputation grows.
“We should be proud of that, not in a narrow way, not with our backs turned to others, but proud to be generous and outward-looking, proud to share, proud to learn – internationalist, not isolationist.”
The motion to end all Welsh Government international spending, tabled in the name of Blaenau Gwent Caerffili Rhymni’s Reform MS Llŷr Powell, was rejected by the Senedd with 37 members for and 48 against.
The Siambr then agreed Plaid Cymru minister Heledd Fychan’s amendment, which proposed the Senedd “regrets Reform UK’s isolationist approach to Wales’s place in the world” and “celebrates Wales’ reputation as an internationalist, tolerant and outward-looking nation open for business, which is enhanced by its international engagement, including spending.”
The amended motion was agreed with 48 in favour and 37 against.



Charity15 hours ago
Toy Story fans fill charity toy box at Haverfordwest cinema
Donations pour in for SNAP Specialist Play as families embrace Toy Story 5 launch A TOY STORY-themed charity appeal at...


Community20 hours ago
Lord Rhys emerges from the mist in St Davids
Giant puppet begins historic journey marking 850 years since the first Eisteddfod MIST swirled around St Davids Cathedral on Friday...


News2 days ago
Tragic tribute paid to Haverfordwest man after A4075 collision
FAMILY REMEMBERS “KIND AND LOVING” CALLUM HANSON THE FAMILY of a 22-year-old man from Haverfordwest who died following a road...


News3 days ago
Motorcyclist, 22, dies in A4075 crash in Pembrokeshire
A 22-year-old woman remains in hospital after two-vehicle collision A MOTORCYCLIST has died following a serious two-vehicle crash on the...


Community3 days ago
Why police will be visiting every home in Pembrokeshire
New operation aims to knock on more than 257,000 doors across Dyfed-Powys over the next three years DYFED-POWYS POLICE has...


Crime3 days ago
Prisons at breaking point: MPs warn Wales is paying the price of a failing system
Frozen healthcare budgets, overcrowded jails, homelessness on release and mounting pressure on staff are undermining rehabilitation across Wales, according to...


News3 days ago
Brexit at 10: How Britain was sold a dream that cost us dearly
A decade after the referendum, the promised benefits remain hard to find while the economic costs are increasingly difficult to...


Crime4 days ago
Worcestershire man jailed after violent attack on woman in Tenby
Defendant was already serving a suspended sentence when serious assault took place A WORCESTERSHIRE man has been jailed for more...


Climate4 days ago
Offshore wind ‘could bring new generation of jobs to Milford Haven’
Pembrokeshire ports and Celtic Sea projects placed at centre of Wales’ green energy ambitions MILFORD HAVEN and Pembroke Dock could...


Community4 days ago
Police officer hailed hero after midnight sea rescue in Milford Haven
PC swam 100 metres offshore to save distressed woman heard calling for help in darkness A DYFED-POWYS POLICE officer has...
-

 Community6 days ago
Community6 days agoPembrokeshire Chess Club crowned Welsh champions
-

 Crime3 days ago
Crime3 days agoMilford Haven man jailed for breaching domestic violence protection order
-

 Local Government5 days ago
Local Government5 days agoSecurity privately arranged by Mayor at Beating of the Bounds
-

 News3 days ago
News3 days agoCrash on Freeman’s Way causes school-run chaos across Haverfordwest
-

 Crime4 days ago
Crime4 days agoMan wanted by court after failing to attend hearing over alleged shop thefts
-
 Crime4 days ago
Crime4 days agoMan banned from roads after drink-driving offence
-

 Crime4 days ago
Crime4 days agoMan jailed after admitting strangulation and assaults
-

 Crime4 days ago
Crime4 days agoMan sentenced over stalking campaign and lock knife offence